


Do you need to check the inside of your vag and derriere?
i.e. Is internal work necessary for pelvic floor health?!

At my most recent yoga studio workshop, I hammered home two seemingly opposing themes:
You have no business telling someone how to engage their pelvic floor if you’ve never felt it, and…
The pelvic floor is part of a bigger system, so treat it as such.
I hear a lot on the pelvic floor internet about whether or not internal work is necessary to treat the pelvic floor. There is one camp that finds it absolutely essential (see point 1), and another that finds that paradigm silly, given point 2.
Both of them, IMO, are true. It’s non-dualism at its best. So let’s cut through the noise and help you figure out whether or not you need internal work

Here’s the tl;dr:
Both vaginal and rectal exams offer specific insight into the musculoskeletal health of the pelvic floor. Nothing can replace that.
However, we can make excellent assumptions about the pelvic floor based on the broader picture.
Nervous system regulation and physical safety is always paramount, so if you don’t feel great about doing an internal assessment, it’s not worth doing! Do not tough it out.
While there is a time and place for specific internal tissue work, any solid pelvic floor rehab should include (or skew heavily towards) movement and nervous system regulation strategies. For the right person, completely external and/or virtual care can be empowering and successful!
Related reading:
Personal training and pelvic floor therapy: Let’s be friends? If you’ve ever wondered, should I be doing personal training, pelvic floor therapy, or both? Here’s your answer via a conversation with the brilliant
!Deadlifts, lunges, and squats, oh my! On how lifting is a superfood for the pelvic floor.
What the hell even IS the nervous system? But also — nervous system regulation trumps all in the pelvic floor world! Don’t skip this!
The deep dive:
Come with me on this corny imagery journey: Whether you’re a human seeking pelvic floor rehabilitation support or you’re a clinician trying to help folks, you now have a toolbox in front of you.
I am not very handy, but I can recognize that screw drivers are pretty fucking important for like, a myriad of tasks. I even know how to use one. If you don’t have a screw driver, or even the right kind of screw driver, there are some tasks you just won’t be able to do.
But should you only have a screw driver in your toolbox? Obvs not. In fact, the best toolboxes, owned by all of my masc of center lesbian pals, are full of delightful devices I have no idea how to use. That’s why they’re always invited to my house at all times, but I digress.
Hammers, drills, etc. — equally if not more important tools. They’re all essential. And the more complicated the situation, the more specialized and varied tools are necessary.
Pelvic floor cases are basically the same.

First, let’s flesh out the counter-argument for internal work: They’re really not looking at the whole picture.
When I was first taught to treat pelvic floor conditions, the vibe was very vagina-centric. Basically, the idea was to do internal treatment every session, either releasing the tissue or coaching folks on kegels.
This gets very boring very quickly. and the results are kind of meh.
As I have written about rather extensively, the pelvic floor is a whole bodymind affair. From a biomechanical perspective, I’m looking at feet, the ability to hinge, upper body strength, rotation, glute strength — the list goes on.
But wait! Your brain and nervous system are a huge part of the party too. This is relevant in all arenas of pelvic health (and fuck it, physical health as a whole, IMO), including urge incontinence, prolapse, and of course, pain. If you’re operating from a constant “fight, flight, or flee” sympathetic state in your movements (i.e. constantly guarding while you pick up your kid so that you don’t pee yourself, for example) that’s going to have a real, physical effect on your pelvic floor and bladder muscles. (Tl;dr, they’re more likely to spasm, making you leak.) For folks with a primary complaint of pain, creating a foundational experience of physical safety in movement is the cornerstone of recovery.
This is why virtual and/or exclusively external work can be so transformative and effective. If your clinician integrates your pelvic floor symptoms as one piece of a bigger whole, and treats the drivers of those symptoms, you’re going to get great results!
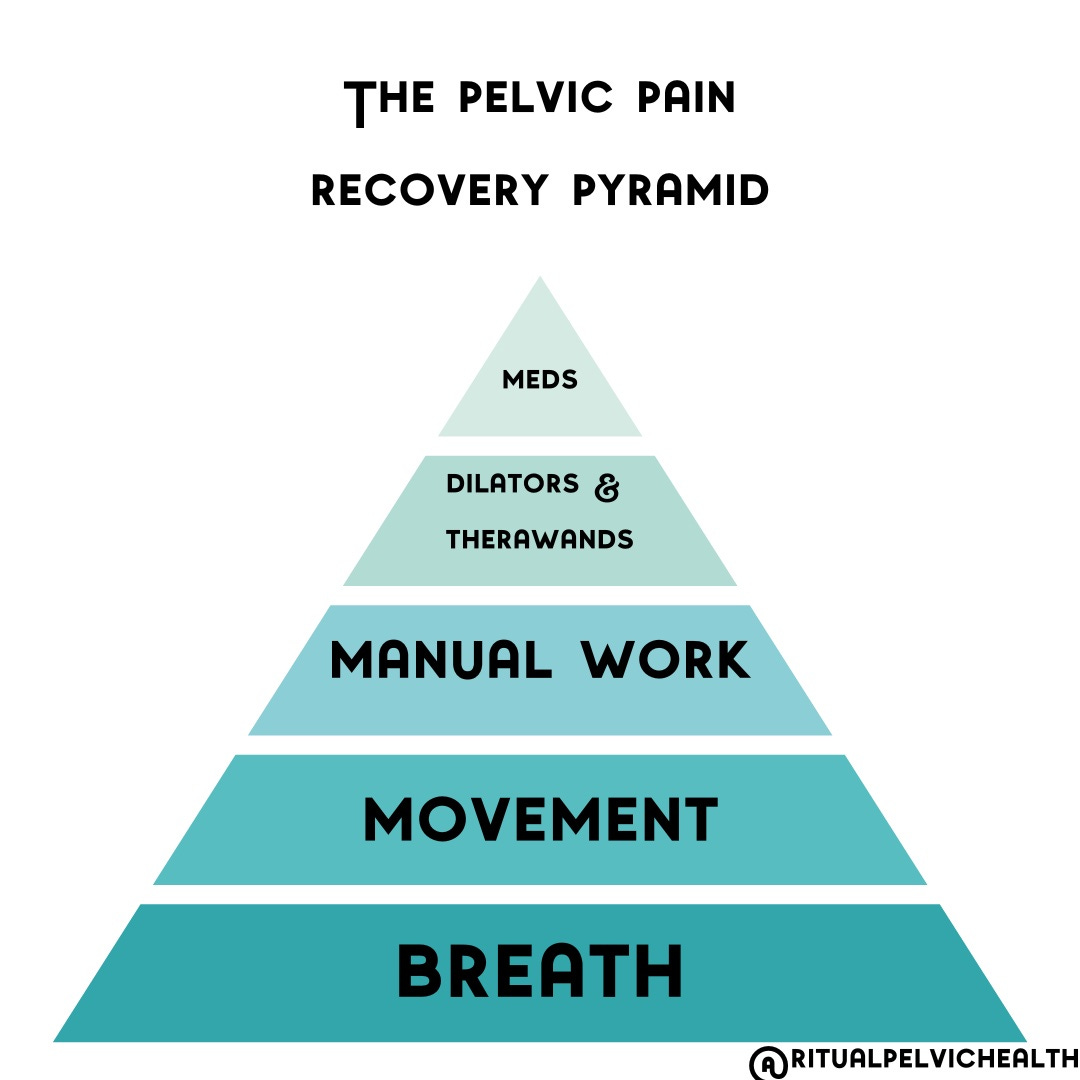
Further, I’m a huge believer in self-efficacy when it comes to physical rehabilitation, because it feels like shit to rely on a provider doing something to you. Instead, my goal as a provider is to facilitate an environment where we get to learn about the client together, understand what works best for them, and create a space where the client becomes more confident using the tools that work best — whether that’s a deadlift, breathing drill, or deep listening strategy. Here’s my visual on treating pelvic pain clients:
And lastly — you can make a huge difference on the pelvic floor doing external manual therapy. I personally love working on the sacrum, all over the pelvis, and the abdomen, and I find that not only does this approach get stand-alone awesome results, but if we do decide that internal work is appropriate, external manual work makes the internal stuff easier and more effective.
Okay! So hopefully I’ve made it clear that the emphasis of pelvic floor treatment should be on the bodymind system as a whole and in context of whatever concerns are arising. Which leaves us with the question of why the fuck we’d ever want to do an internal exam in the first place.
It’s pretty simple, tbh. Internal assessments and treatment give you information and opportunities you wouldn’t get otherwise.
At this point in my career, I’m pretty good at guessing what I’ll feel on an internal assessment based on intake alone. But! I am still surprised on occasion — and those surprises change my treatment plan.
Internal work gives a clinician an opportunity to learn about their client more thoroughly. And while the pelvic floor can be influenced hugely by movement, direct manual work to the pelvic floor tissue can sometimes be the most efficient way to introduce change, and therefore communicate that change is possible to a client’s nervous system.
Frequently with my in-person clients, I begin with manual work to create change and then transition to movement strategies to make it empowering and sustainable. Internal check-ins are helpful to gauge progress from time to time, or to teach and/or reinforce specific skills (like how to use breath to release the pelvic floor, or how to do a proper kegel if appropriate), but those checks are not the bread and butter of the treatment plan.
The big caveat here is that if the phrase “internal work” makes your pelvic floor snap shut, or even if it just makes you uneasy, then it’s off the table. Felt safety is the number one priority, and any internal work that feels physically painful or just increases anxiety isn’t productive. There is so much more a skilled therapist can do outside of internal work, and while it’s it’s a great tool, it’s not the right tool to use in these circumstances. If you’ve ever had a provider tell you that you can’t make progress without internal work, fire them. (Strong opinion, sorry not sorry!)
Here’s the take-home:
So, do you need internal work? I don’t know, because I don’t know your story!
But in general, a mixed modality, multi-tool approach is my favorite. Use the right tool at the right time!
On Thursday, I’ll be publishing a self-assessment to help you figure out if pelvic floor therapy might be a thing worth pursuing, and if internal work could be supportive. If you’re not already a paid subscriber, you can fix that here:
Until then, I love hearing from you. Reply to this email or comment below to share your story, ask a question, or post feedback!
As always, I am rooting for you.
Hi Cait! I’ve been wanting to schedule an in-person appointment but can’t figure out how to on your website. It seems like all links go to virtual.
I’m looking forward to Thursday!